Most families don’t learn the difference between hospice and palliative care until it’s urgent. Here’s what you need to know.
Most people learn the difference between palliative care and hospice in the worst possible moment: sitting across from a doctor, trying to absorb a diagnosis, while words like “comfort-focused” and “goals of care” float past them unexplained. The confusion is so common that researchers have a term for it, prognostic awareness gaps. And it has real consequences. Families who don’t understand these two types of care often delay both, missing weeks or months of support that could have made an enormous difference.
This confusion is not uncommon. Most people encounter the terms hospice and palliative care for the first time during one of the most stressful seasons of their lives, and the medical system rarely slows down long enough to explain the distinction properly. So what is the difference between hospice and palliative care? And which one may be right for your loved one?
Understanding the difference between hospice and palliative care isn’t just a matter of semantics. It can shape what treatments your loved one receives, what support your family gets, and what the days ahead might look like. The good news: once you understand how each works, the path forward often feels a little less uncertain.
What Is Palliative Care?
Palliative care is specialized medical care focused on relieving symptoms, pain, and stress caused by a serious illness. The goal is straightforward, even if the name sounds clinical: help the patient feel better, so they can live as fully as possible. That will look different for everyone.
What makes palliative care distinctive is that it runs alongside curative treatment. A person with cancer who is actively receiving chemotherapy can also receive palliative care. Someone managing heart failure while still pursuing aggressive treatment can benefit from a palliative care team. It is not a signal that treatment has stopped or that hope has run out. It is simply a recognition that managing suffering matters just as much as fighting disease.
Palliative care teams are typically interdisciplinary. That means a physician, nurse, social worker, and sometimes a chaplain or counselor working together to address the full picture of a patient’s experience, not just the illness itself, but the anxiety surrounding it, the financial strain, the family dynamics, and the questions about what comes next.
What Conditions Qualify for Palliative Care?
Palliative care is appropriate for virtually any serious illness at any stage. Common conditions include:
- Cancer (at diagnosis, during treatment, or in advanced stages)
- Congestive heart failure
- Chronic obstructive pulmonary disease (COPD)
- Kidney disease
- Alzheimer’s disease and other forms of dementia
- Parkinson’s disease
- Stroke
- ALS (amyotrophic lateral sclerosis)
Age is not a limiting factor. Children with serious illnesses can receive palliative care just as adults can. And importantly, there is no requirement that a person have a terminal diagnosis or a specific life expectancy to be eligible for palliative care.
What Does Palliative Care Actually Do?
Palliative care addresses symptoms that too often go undertreated in conventional medical settings. Pain is the most obvious, but palliative teams also work on:
Breathlessness – one of the most distressing symptoms a person can experience, and something palliative specialists are specifically trained to manage.
Nausea and appetite loss – particularly common during cancer treatment, and deeply affecting to witness in someone you love.
Fatigue – which is far more layered than ordinary tiredness and often needs targeted intervention.
Anxiety and depression – serious illnesses almost always carry an emotional weight, and palliative care explicitly acknowledges and treats this, rather than leaving it to chance.
Communication and decision-making support – palliative teams help patients and families understand complex medical options, clarify goals of care, and navigate difficult conversations about the future.
Where Is Palliative Care Provided?
Palliative care can be delivered in hospitals, outpatient clinics, long-term care facilities, and increasingly, at home. Many major hospital systems now have dedicated palliative care teams, and access to palliative care has grown significantly over the past decade. That said, availability varies considerably by location and facility. If you’re unsure whether a hospital or treatment center offers it, it’s worth asking directly.
What Is Hospice Care?
Hospice is a specific type of care designed for people who are nearing the end of life. It is generally defined as a prognosis of six months or less if the illness follows its expected course. It is, at its core, a philosophy of care: one that says when curative treatment is no longer beneficial or desired, the focus should shift entirely to comfort, dignity, and quality of life.
Hospice care does not mean giving up. It means choosing a different kind of fight. One that is focused on living well in the time that remains, rather than pursuing treatments that may prolong life at the cost of comfort.
When a person enters hospice, the care model changes significantly. Instead of coordinating care around hospitals and specialists, a hospice team comes to the patient. Most hospice care in the United States is delivered at home, though it is also provided in dedicated hospice facilities, nursing homes, and assisted living communities.
What the Hospice Team Looks Like
Like palliative care, hospice is a team effort. A typical hospice team includes:
A hospice physician oversees the medical plan and communicates regularly with the patient’s primary doctor.
A registered nurse who visits regularly, often several times a week, to manage symptoms, adjust medications, and check in with the family.
A certified nursing aide who helps with personal care like bathing, grooming, and light tasks.
A social worker who addresses practical needs: understanding benefits, coordinating resources, navigating family dynamics, and helping with advance care planning.
A chaplain or spiritual care coordinator who offers non-denominational support around meaning, grief, and whatever the patient and family find meaningful.
A bereavement counselor who supports the family, not just during the patient’s final days, but for up to 14 months after their death.
This last point is worth sitting with. Hospice care doesn’t end when the patient dies. The bereavement support it provides to surviving family members is one of the most underappreciated gifts of this type of care.
How Is Hospice Paid For?
In the United States, hospice care is covered by Medicare Part A, Medicaid, and most private insurance plans under what’s called the Medicare Hospice Benefit. To qualify, a patient must have a terminal illness with a prognosis of six months or less (certified by two physicians), and they must agree to forgo curative treatment for the terminal illness. However, they can continue to receive treatment for unrelated conditions.
The Medicare Hospice Benefit covers a broad range of services: medications related to the terminal diagnosis, medical equipment (hospital beds, wheelchairs, oxygen), nursing visits, aide services, and the interdisciplinary team support described above.
One common concern families have is whether choosing hospice means the person can’t change their mind. They can. A patient can leave hospice at any time. If their condition improves, if they decide to pursue treatment again, or simply because they change their minds. The decision is not permanent.
Hospice vs Palliative Care: The Core Differences
If you’ve been reading carefully, you may already sense where the lines fall. Here is a clear summary of the key differences:
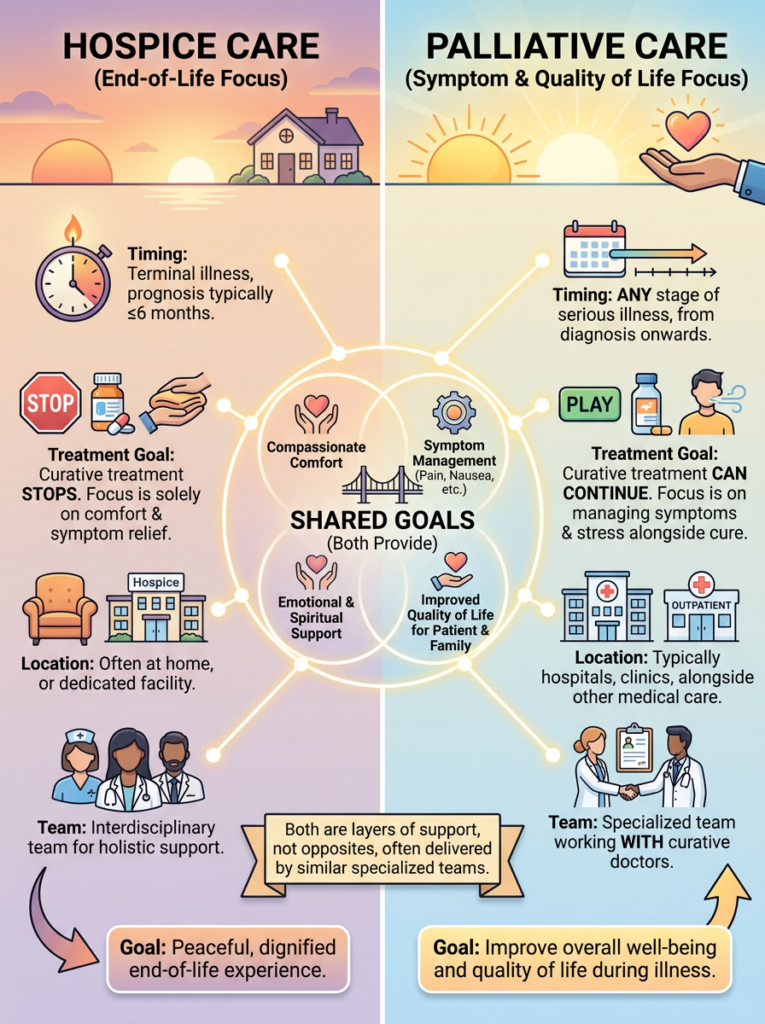
Timing and prognosis. Palliative care can begin at any stage of a serious illness, even at diagnosis. Hospice is specific to the end of life, when a prognosis of six months or less has been established.
Treatment approach. Palliative care is provided alongside curative or life-prolonging treatment; the two are not in conflict. Hospice care requires that the patient forgo curative treatment for the terminal illness, though comfort-focused treatments continue.
Setting. Palliative care is often hospital-based or provided through outpatient clinics, though home palliative care is growing. Hospice care is primarily home-based, with additional options in hospice facilities and long-term care settings.
Who pays. Palliative care is typically billed through standard insurance like any other specialty visit. Hospice is covered as a specific benefit under Medicare, Medicaid, and most private plans.
Duration. Palliative care has no time limit and can continue for years. Hospice is certified in 90-day periods (two initially, then 60-day periods after), though it can continue as long as the patient remains eligible.
Focus. Both care types prioritize comfort and quality of life, but palliative care balances that with ongoing treatment goals, while hospice centers focus exclusively on comfort.
Which Type of Care Does Your Loved One Need?
This is the question that matters most, and it doesn’t have a single right answer. It depends on where your loved one is in their illness, what they value, and what they want their remaining time to look like.
If your loved one has been newly diagnosed or is in active treatment
Palliative care is likely the right place to start. Research consistently shows that patients who receive palliative care alongside treatment report better symptom control, lower rates of anxiety and depression, and, in some studies, notably a landmark 2010 study in the New England Journal of Medicine, even longer survival than those who received standard care alone.
Introducing palliative care early is not defeatist. It is simply good medicine. If your loved one’s care team hasn’t mentioned it, it is entirely appropriate to ask: “Would palliative care be helpful here?”
If your loved one’s condition is progressing and treatment is no longer working
This is often the most difficult moment for families. When a doctor says that further treatment is unlikely to change the outcome, the natural response is to ask: “But is there anything else we can try?” That instinct comes from love. And it’s worth honoring.
At the same time, this is when the hospice conversation is worth having openly. Not because all hope is gone, but because a different kind of hope becomes available. The hope for days at home instead of in a hospital. The hope for managed pain.The hope for meaningful time together, without the exhaustion of treatment schedules.
Many families say, looking back, that they wish they had called hospice sooner.
If your loved one is still pursuing treatment but struggling with symptoms
This is exactly the space palliative care was designed to fill. Pain, nausea, breathlessness, and anxiety don’t have to be endured as an unavoidable part of being ill. A palliative care referral can run parallel to whatever treatment is underway.
How to Start the Conversation
If you’re not sure which direction is right, the best first step is a family meeting with your loved one’s primary physician or oncologist. Come prepared with honest questions:
- What is the realistic goal of continued treatment at this point?
- Would palliative care help manage symptoms right now?
- At what point would you recommend we think about hospice?
- What does the next few months look like, realistically?
These are hard questions to ask. But they are also the questions that lead to better care.
Common Misconceptions Worth Clearing Up
“Hospice means the doctors have given up.”
Hospice physicians are specialists in their own right. Choosing hospice doesn’t mean anyone has stopped caring. It means the entire focus of care has shifted to the patient’s comfort and quality of life. Many hospice nurses and doctors describe their work as among the most meaningful of their careers.
“Palliative care is only for people who are dying.”
Not at all. Palliative care is appropriate from the moment of a serious diagnosis, regardless of prognosis. Even someone with a chronic illness who expects to live for many years can benefit from palliative support.
“If I choose hospice, I can’t go to the hospital.”
This is partially true and worth understanding clearly. Hospice does cover some inpatient stays for acute symptom management or respite care. However, the general model is home-based, and emergency hospitalizations for aggressive treatment are outside the hospice benefit. The hospice team can help families understand what situations warrant a call to them versus a 911 call.
“Hospice speeds up death.”
Studies have not supported this, and many suggest the opposite. The comfort-focused care hospice provides may actually allow some patients to live longer than they would have under aggressive treatment. More importantly, it allows them to live better.
Frequently Asked Questions
Can someone receive both palliative care and hospice?
Not simultaneously, in the strict sense. Hospice is itself a form of palliative care, specialized for end-of-life. But many people receive general palliative care for months or years before transitioning to hospice when the time comes.
Can a person leave hospice if they improve?
Yes. If a patient’s condition stabilizes or improves, they can be discharged from hospice and return to curative treatment. They can re-enroll in hospice later if needed.
Does palliative care cost extra?
Palliative care visits are typically billed through standard insurance, similar to any specialist visit. Medicare, Medicaid, and most private insurers cover it, though copays and cost-sharing rules vary. It’s worth calling your insurer or asking the palliative care team’s billing department for specifics.
How do I find palliative care or hospice providers in my area?
Your loved one’s primary physician or specialist is the best starting point for a referral. The National Hospice and Palliative Care Organization (NHPCO) maintains a provider directory at nhpco.org. For hospice specifically, the Medicare Care Compare tool at medicare.gov allows you to search by zip code and compare local providers.
What if my loved one refuses hospice?
This is more common than many families expect, and it deserves respect. Hospice requires the patient’s consent. If your loved one isn’t ready for that conversation, it doesn’t have to happen today. A palliative care referral can be a gentler entry point, and sometimes, after working with a palliative team for a period of time, patients become more open to the idea of hospice when the moment is right.
Is there pediatric hospice or palliative care?
Yes. Children with life-limiting conditions have access to specialized pediatric palliative care programs, which address the very different emotional and practical needs of families with seriously ill children. Unlike the standard Medicare hospice benefit, children enrolled in Medicaid can typically receive both curative treatment and hospice simultaneously, which is an important distinction from adult hospice rules.
Navigating serious illness on behalf of someone you love is one of the hardest things a person can do. The decisions feel enormous, the timeline is uncertain, and the medical system can feel impersonal at exactly the moment when you most need it to feel human.
Understanding the difference between hospice and palliative care won’t make those decisions easy. But it removes one layer of fog from a path that’s already hard to see. Both types of care exist because people recognized that suffering doesn’t have to be part of illness, and that dying well is something worth pursuing intentionally.
Whatever stage your family is in, there is care available that is designed specifically for this season. You don’t have to figure it out alone.
For more information, read on:
7 Surprising Facts Hospice Nurses Want You To Know
Sources:
Medicare Hospice Benefit — Eligibility & Benefit Periods Centers for Medicare & Medicaid Services. Medicare Hospice Benefits (official booklet). → medicare.gov